
It was early in their courtship seven years ago when Manuel Villanueva warned his now-husband, “I come as a package of three.”
The other parts of that deal: his father, Ramon Villanueva, whose failing kidneys forced him to stop working, and his mother, Maria Guadalupe Olague.
Now they live as a family unit of four — six, if you count the cats — in a Highland Park two-bedroom apartment. As caring for his parents has increasingly taken a toll on his finances, time and psyche, Manuel Villanueva has taken up a matter-of-fact mantra to soldier on: “Adapt and understand your reality.”

California, too, must adapt to its reality. The state’s long-held self-image — a blend of Tomorrowland and Fountain of Youth — is colliding with the inescapable fact that the Golden State is getting old.
The next governor will be confronted with a demographic shift of epic proportions: Seniors will be California’s fastest-growing population. Between now and 2026, the number of Californians 65 and older is expected to climb by 2.1 million, according to projections by the state Department of Finance. By contrast, the number of 25- to 64-year-olds is projected to grow by just more than half a million; the number of Californians younger than 25 will grow by a mere 2,500.
Seniors to shape California’s future
According to projections from California’s Department of Finance, seniors will make up a sharply larger share of the state’s population by 2060 — the only age bracket to grow in scale.


That radical transformation has been largely absent from discussion as politicians grapple with education, healthcare and environmental policies.
But the graying of California will seep into nearly every nook of the state budget and policy planning under the next governor. It will determine what services will be in demand and how money must be spent. Most significant, it will place enormous strain on the state’s already fragile network of long-term services and supports, including in-home aides and skilled nursing facilities.
“We are exquisitely unprepared for that [oldest] age demographic pushing through,” said Dr. Bruce Chernof, president of the SCAN Foundation, an aging advocacy group.
‘Things are going to be dramatically changing’
What does it mean to govern an aging state? It means dealing with higher healthcare costs, particularly for low-income seniors who are eligible for Medi-Cal coverage, the state-subsidized healthcare system for the poor. There are currently close to 1.2 million Californians 65 or older enrolled in the program.
It means grappling with poverty in a different way. California politicians often focus on the state’s child poverty rate, which averaged nearly 23% from 2014 to 2016. But fewer talk about the poverty rate among seniors, which was 20% during the same time period, according to the U.S. Census Bureau’s Supplemental Poverty Measure. The fastest-growing population of homeless people is among older adults; in Los Angeles County, the number of homeless people 62 or older surged by 22% this year, even as the overall homeless population slightly dropped.

As the population of low-income seniors swells, demand for safety-net programs for the elderly — such as financial assistance for low-income seniors or payments to in-home caregivers — is likely to balloon.
State coffers, as well as local governments and school districts, could be squeezed by growing numbers of retired government workers. Even best-case scenarios show the state could need an additional $230 billion over the next three decades for existing promises to cover retirees’ pension and healthcare costs.
It could mean revamping the transportation system to better accommodate people who can no longer drive, or making sure more units of new housing are accessible to people in wheelchairs or with impaired mobility. Is air quality an aging issue? Yes, particularly when incidents of asthma, commonly seen as a childhood disease, increase among those over 65.
And with projections showing that California’s population will skew older for decades to come — beyond the baby boomer generation — the decisions the next governor makes could reverberate for the foreseeable future.
A rapidly aging state
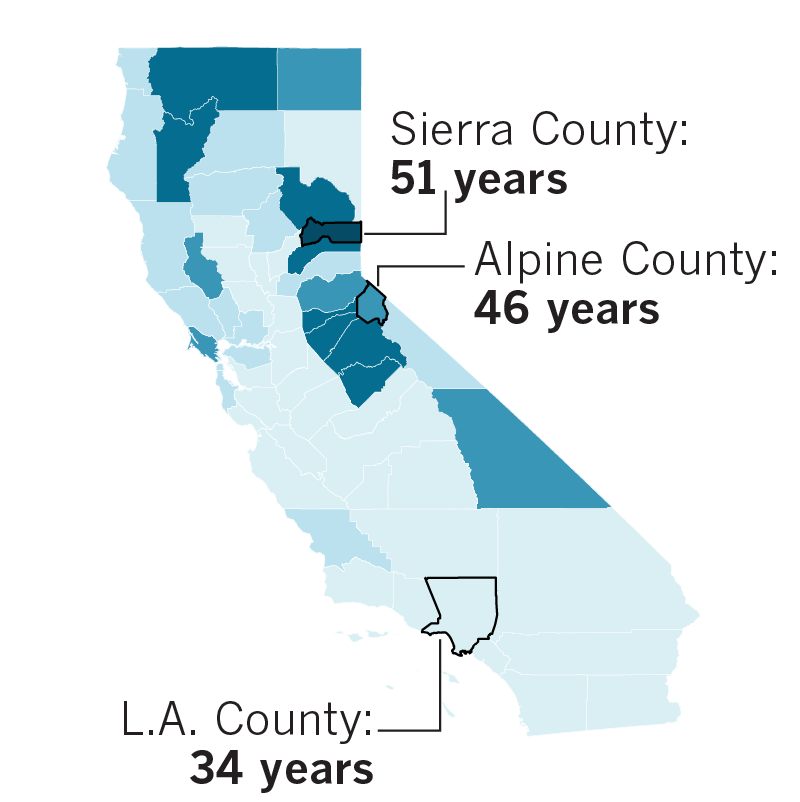
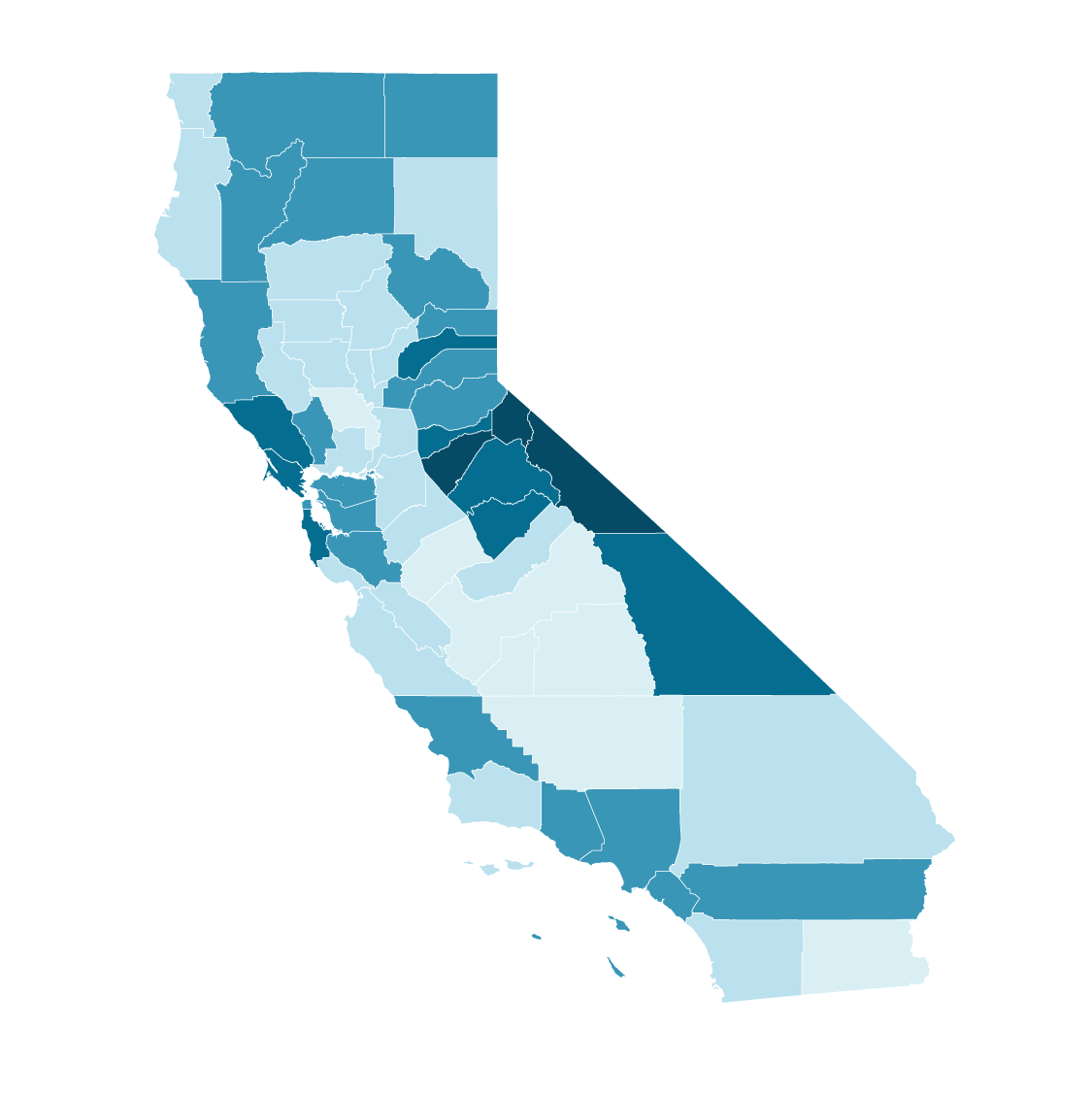
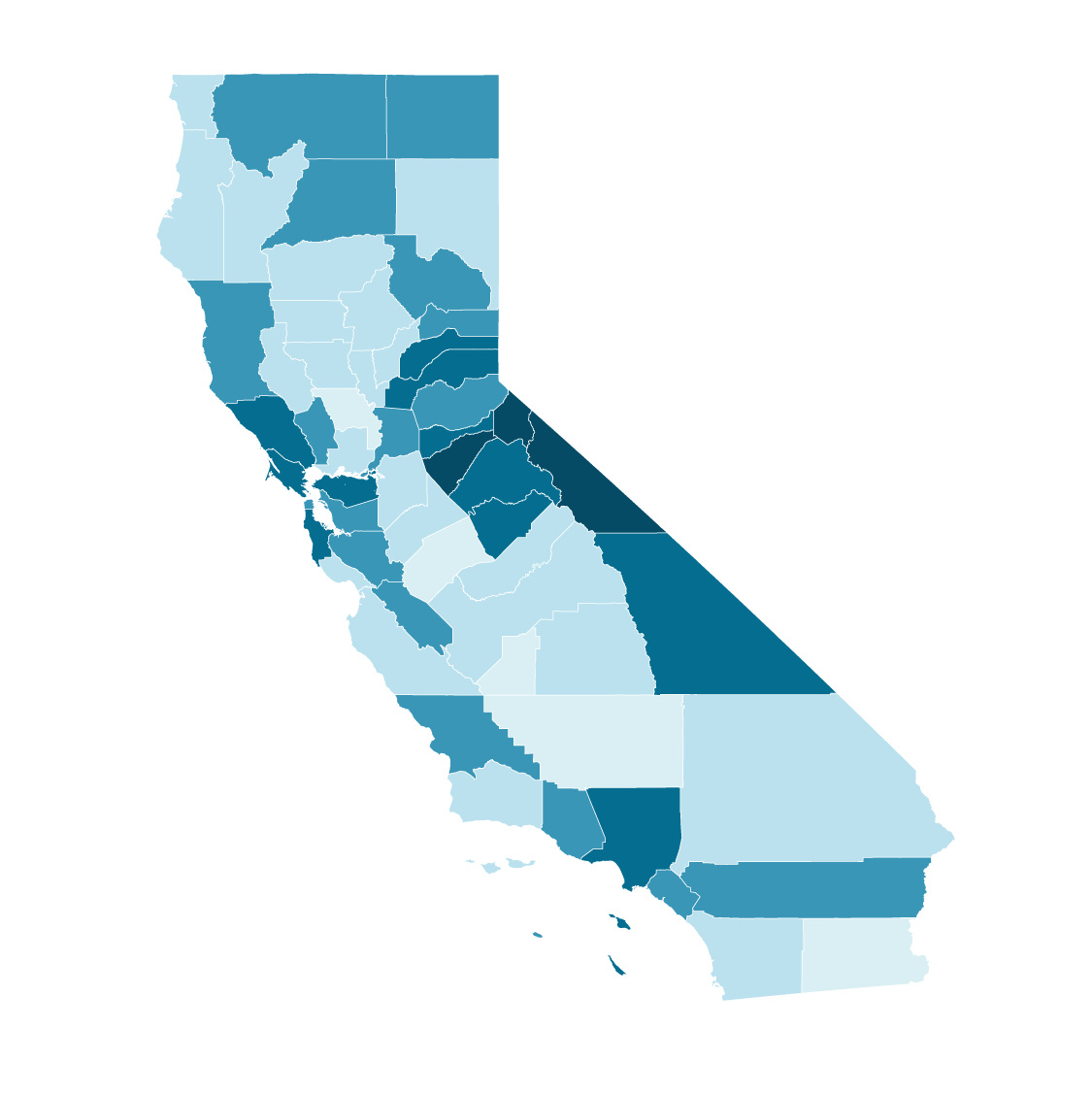
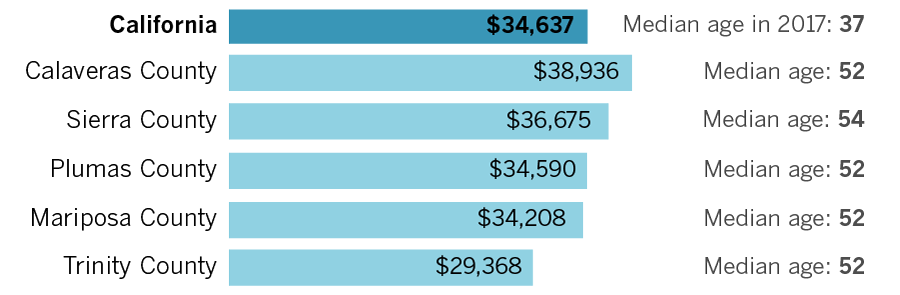
Almost every county in the state will see its median age rise more than five years by 2050. Many of the counties with the highest increases are in rural, more sparsely populated areas.
Median age in California counties



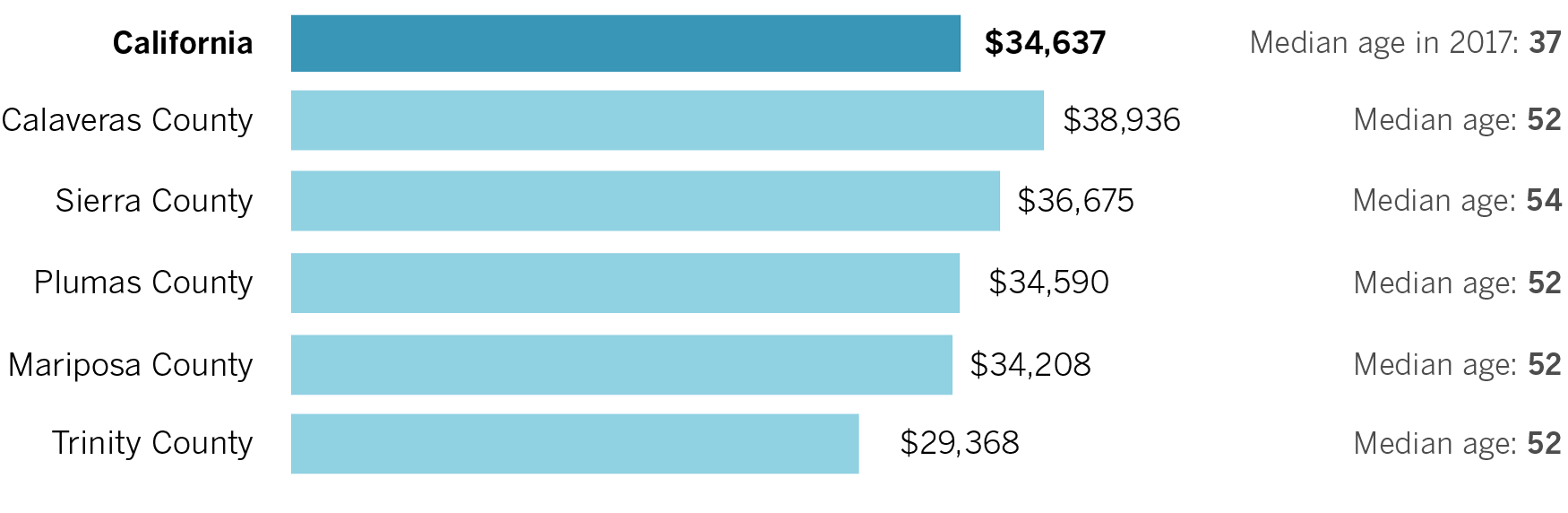
Median income in California’s oldest counties
“If we have that conversation based on the demographic makeup of what the state is today, and we don’t anticipate things are going to be dramatically changing over the next several decades, we’re not going to be prepared to make the right decisions,” said Paul Rosenstiel, chairman of the board of the California Budget and Policy Center.
No single government entity has ownership of the issue of aging. Medi-Cal is governed by the Department of Health Care Services, while the In-Home Supportive Services program, which pays for home care for the low-income elderly and disabled, is overseen by the Department of Social Services and is administered by each county. The Department of Aging contracts with local agencies to provide caregiver resources, while the Department of Veterans Affairs operates homes for aging vets.
“It’s like a hundred-piece jigsaw puzzle,” Chernof said. “None of those departments and funding streams have much connection to each other.”
A ‘jigsaw puzzle’ of resources
Navigating government-provided resources available to California’s seniors can be confusing. Here’s a starting point.
Medicare: The federal healthcare program for seniors (doesn’t cover long-term care).
Medicaid: The federal program provides health coverage to low-income seniors. About 8.3 million seniors are enrolled in both programs.
Medi-Cal: California’s Medicaid program, which covers long-term care.
California Department of Aging: Provides resources to caregivers and seniors.
California Department of Veterans Affairs: Operates homes for aging vets.
In-Home Supportive Services: Pays for home care for Medi-Cal eligible seniors and disabled people.
Despite their universality, aging issues have never inspired much of a political rallying cry. In part, Chernof said, that’s because they force people to contemplate their own mortality — never an easy sell — and also offer little immediate upside.
“Aging is slow-motion,” he said. “Fixing a pothole today is something everybody can see and feel. Improving how aging programs work with each other feels really invisible until you get that call [that] Mom fell and broke her hip, and she’s not going to be able to go back to her apartment because it’s a second-floor walk-up [and] she can’t walk upstairs anymore.”
It’s been especially difficult for advocates to shake off the sense that caring for the elderly is a family matter, not one of statewide concern. Donna Benton, professor of gerontology at USC, said the strain that aging can cause for seniors and their families has long been seen as “a private affair.”
“But domestic violence used to be considered a private affair,” Benton added. “This is a public health issue now.”
A fragile network
Luck isn’t often associated with Alzheimer’s disease. Yet when Maggie Ownbey, 61, and her younger sister Sue Ownbey-Menaker reflect on caring for their mother, Eleanor, they focus on their good fortune.
Ownbey-Menaker happened to get her teeth cleaned one day by a dental hygienist whose father also had the disease. The hygienist told her that she used the suction machine — a staple in dental offices — to clear out blockages if her father had trouble swallowing. The sisters got a machine to keep in their mother’s Burbank home, and it saved her life one day when she began choking.
The biggest break was when their father left his life savings to his wife after his death in 2004. He probably envisioned his wife using that money to live comfortably in retirement. Instead, after her 2006 Alzheimer’s diagnosis, their nest egg went entirely to her care.
At first, the sisters hired someone to spend a few hours with their mother during the day, but in the nearly four years before her death in 2014, it was round-the-clock.
The high cost of aging in California
$116,000: Median yearly cost for a private room in a nursing home
$57,200: Median yearly cost for a home healthcare aide
$2,956: Average basic monthly living costs for an older couple (with a mortgage)
$3,700: Average annual premium for long-term care insurance for a 65-year old couple
$11: Average hourly wage for In-Home Supportive Services workers
“I’m just grateful that it was there,” Ownbey-Menaker said of her father’s savings. “I just kept thinking, ‘We should be in Ireland, Mom. We should be on a cruise.’ I hated writing checks to pay for caregivers.”
The money helped — paying $17 to $24 an hour adds up quickly. But it didn’t absolve the sisters of dedicating their time to her care, and to hours upon hours researching the disease and interviewing potential caregivers. Without a road map on how to navigate the complexities of care, they relied mainly on Google and Alzheimer’s support groups to solve whatever was the crisis of the moment for their mother as well as Ownbey-Menaker’s mother-in-law, who battled the disease at the same time.
“We didn’t have a starting point,” Ownbey said. “We had to figure it out like a DIY kit.”
The sisters have since thrown themselves into advocacy, lobbying the federal government for research money for a cure. But they said the state also has a role to play in supporting caregivers to make sure they can easily find the information they need.
Maybe then the next family whose mom has trouble swallowing won’t need to bank on fortuitous advice from their dental hygienist.
By many measures, California is not ready to meet the demand for long-term care. Just under 2% of residents are insured for it, according to the state Department of Insurance. A 2014 poll found that just 3 in 10 Californians over age 40 felt very confident about their ability to pay for future care. And the Employment Development Department projects that the state will need 250,000 more personal care aides by 2026, a growth rate of 40%.
Nancy McPherson, the California state director for AARP, said long-term care is the No. 1 issue for the retiree advocacy group.
“It’s not enough to have service delivery,” McPherson said. “You need to have a coordinated system, and you need to have a means for middle-income Californians to get the support they need.”
Though wealthy Californians can rely on long-term care insurance or ample savings and the poorest can qualify for safety-net programs, the middle class is especially vulnerable when it comes to paying for care. The out-of-pocket costs can be staggering, and Medicare, the federal healthcare program for seniors, does not cover long-term care. A 2017 survey by Genworth, a long-term insurance company, found the average yearly cost for a home healthcare aide was $57,200. The median cost for a private room in a nursing home was more than $116,000.
“You are depleting generational wealth, ensuring it is not passed down,” said Kristina Bas Hamilton, legislative director of United Domestic Workers, a union of home care providers. “You are essentially demolishing the American dream of the kids doing better than the parents.”

Turning to unpaid caregivers can force healthy family members to drop out of the workforce in order to give care full time. A 2015 AARP study found that the 4.5 million family caregivers in California provided $57 billion worth of unpaid care — roughly the equivalent of the gross domestic product of Costa Rica.
Lower-income Californians have some relief through Medi-Cal, which covers long-term care — including an estimated $13 billion in costs this fiscal year for nursing facilities and home-based aides. A key part of that safety net is the state’s In-Home Supportive Services program, which advocates for the aging credit with enabling seniors and disabled residents eligible for Medi-Cal to stay in their homes and receive paid care, usually from a family member.
But the $11.6-billion program, which is jointly funded by the federal government, the state and counties, has been a frequent subject of recent budget squabbles. The cost of IHSS, like other social services programs, is partly driven by caseload — as long as someone meets the eligibility requirements, they’re entitled to care. Caseload has increased by 30% in the last 10 years, and funding out of the state’s general fund has nearly doubled in that time, driven by clients needing more paid hours of care as well as minimum wage and overtime pay for workers.
“We could have the best governor in the world, the friendliest governor in the world,” Bas Hamilton said. “At some point, the general fund can’t support this program. At some point, the program is just not sustainable.”
The spiraling costs are just one reason for concern. Advocates for the program say it is increasingly difficult to find enough caregivers to meet participants’ needs, even when a county determines a client is eligible for a set number of hours of care.
“There is no region in the state of California where demand is met,” said Laphonza Butler, president of Service Employees International Union Local 215, which represents IHSS workers. “Every county has thousands of unused authorized hours. What that says to us is there are California residents who need services but can’t find a caregiver to help them.”
The reasons for shortages vary: In urban areas, it’s the high cost of living, while in rural areas, it’s hard to find people with cars who can travel longer distances. And the low wage paid to caregivers — an average of $11 an hour for IHSS workers — is an obstacle everywhere.
“Who on Earth is going to do this job for essentially minimum wage?” Bas Hamilton said. “You could go work at Starbucks and have a lot less stress in your life. The paradox of our society is we pay the least to take care of the people we love.”
‘This has been devastating’
Susan Lowry never liked the idea of government social programs. She thought they were for moochers, a term she now says with a cringe.
But then she noticed her husband, Alan, was forgetting the names of major streets and struggling to find words. That was seven years ago. It took 18 months for him to be diagnosed with frontotemporal dementia, a rare degenerative brain disease. Eventually she had to stop working as a freelance deposition reporter; the hours were too unpredictable as Alan needed more care.
Soon she was losing the vestiges of their old life together — the boat, the motor home, the yearly ski passes. She sold their home in El Dorado Hills, near Sacramento, so she could be closer to family in northern San Diego County.

“Do I really want to put a number on it?” she said when thinking of all the costs. “It’s more than a number. This has been devastating. Your whole life is just burnt to the ground.”
The saving grace, she said, has been the programs she once disdained. Alan was eligible for a special Medi-Cal program for the working disabled, which allowed Susan, 54, to keep their house and retirement account. She became his IHSS worker, which enables her to care for him full time. A local nonprofit group, funded by government grants, offers respite services — a volunteer caregiver will watch Alan for a few hours, letting Susan escape for a bike ride or a trip to the consignment store.
She feels stronger now, though she’s still just barely getting by. Her days revolve around Alan, now 60 — getting him dressed and fed, taking their daily two-mile walks, putting his favorite episodes of “Bonanza” on TV. He’s largely nonverbal now, but on rare occasion he will say her name.
Susan knows that one day she won’t be able care for him full time. But the long-term care options are scarce. In her research, she found just two nursing homes in San Diego County that will take Medi-Cal patients with dementia who pose a wandering risk, as Alan does. Neither have available beds. If Alan’s disease accelerates before a Medi-Cal option is open, she’ll have to tap into her retirement savings.
“Believe me, by no means am I over any kind of hump,” she said. “I’ve got a long ways to go before I can count myself out of this disaster. I can be penniless with no retirement whatsoever at a very young age.”
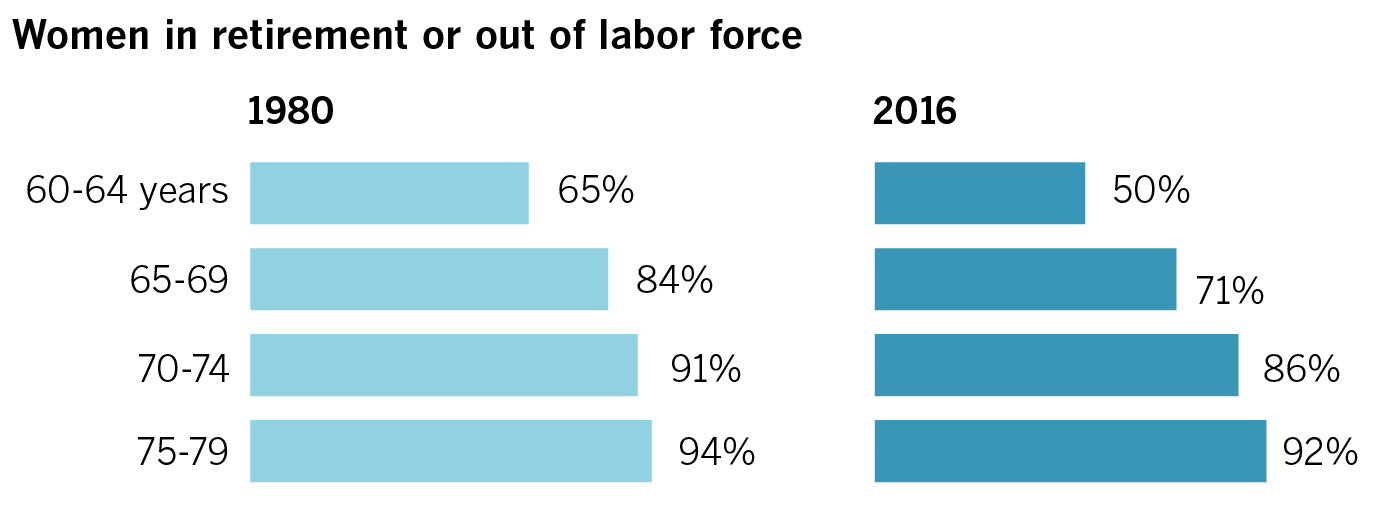
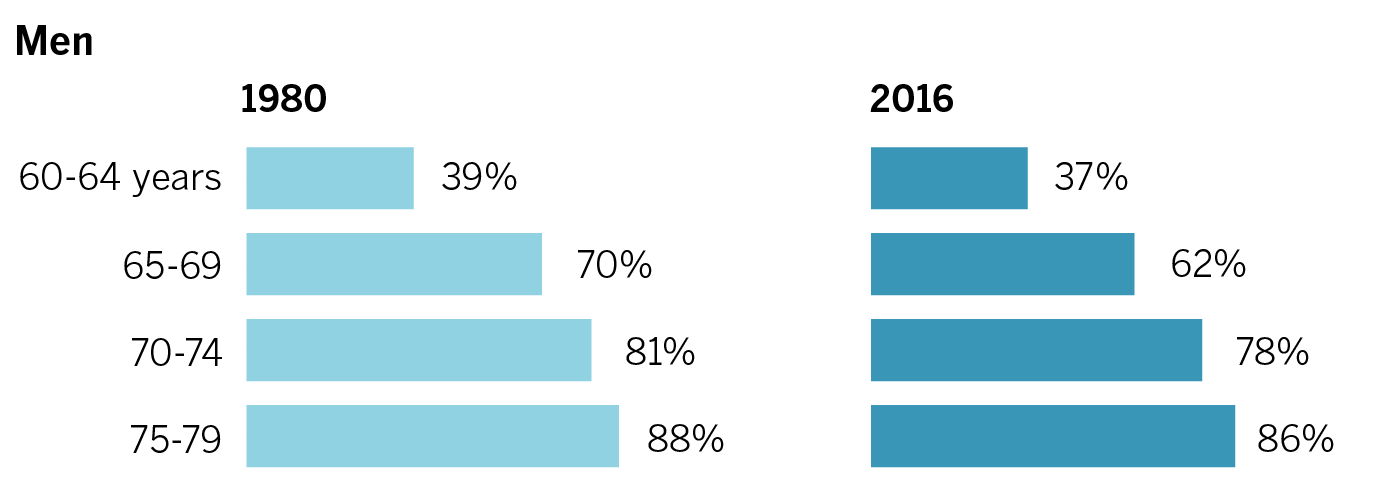
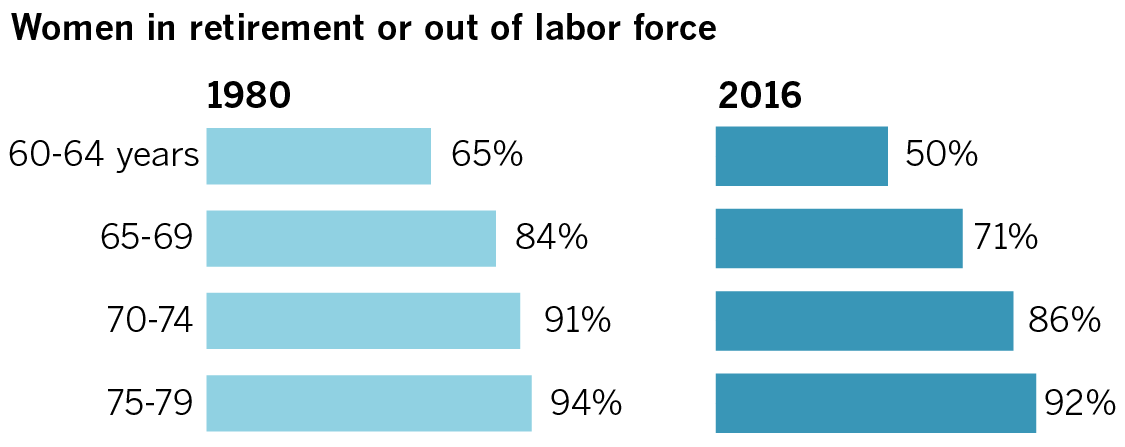
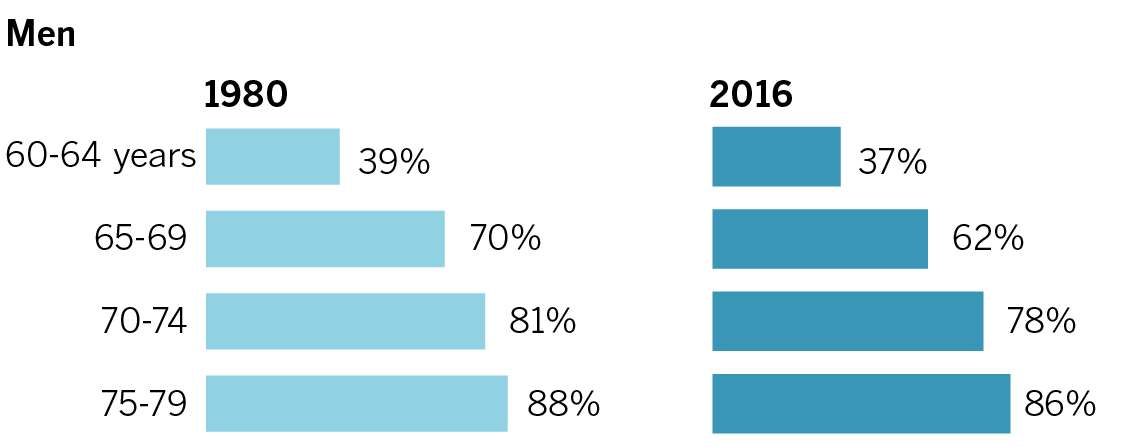
More Californians delaying retirement
Large percentages of women and men are staying in the workforce past their 60s.
The next governor has no choice but to face California’s inevitable demographic shift. But he can choose how he’ll respond.
Some, including Chernof, are pushing for a sweeping state master plan on aging, in spirit of the model crafted in 1960 for the future needs of California’s higher education system.
“It’s laying out a blueprint with a very long time horizon,” Chernof said. “Planning is not based on the cycle of one administration or one election cycle. The idea is that these are issues that will touch every Californian, regardless of who is governor.”
IHSS proponents are contemplating a way for middle-class families to buy into the program. Others propose the state create a type of social insurance program that Californians can pay into and then use the benefits to cover long-term care costs. Alzheimer’s care advocates have proposed a “Care Corps” program to train recent high-school and college graduates to provide non-medical care for seniors with cognitive impairment. Backers of single-payer healthcare have proposed folding long-term care costs into a larger overhaul of the state’s medical system.
Both gubernatorial candidates — Democrat Gavin Newsom and Republican John Cox — have said they support a comprehensive state plan on aging.
Those proposals will have to jockey for money and political will against other demands on the state budget.
“We get a lot of pressure to come with ideas that don’t have a dollar ask,” said Kevin Prindiville, executive director of the advocacy group Justice in Aging. “But we’re going to have to spend some money to solve these bigger problems.”
But there is an upside, said Paul Downey, chief executive of Serving Seniors, a San Diego nonprofit: the large number of people with life experience, expertise and free time to give back to the community in retirement.
“Do we let all of this huge cohort of people falling into that category just retire and go play shuffleboard? They may want to play shuffleboard for the first six months and then get bored,” Downey said.
“The challenge is: How do you use that?” he added. “How do you capture that to better life for everybody?”
Back in Highland Park, Manuel Villanueva’s life revolves around a litany of health problems. Ramon, 69, gets dialysis three times a week and has dementia, while Maria Guadalupe, 65, has diabetes.
Both parents are covered by Medi-Cal, which also pays for Ramon’s transportation to and from dialysis treatments. Villanueva has considered using the state’s paid family leave protections — which apply to caregivers as well as new parents — to aid in attending to his parents, but so far the burden has largely been his own.
It’s enough to test the limits of Villanueva’s mantra.
“Even though I adapted to my reality, I feel very cornered sometimes,” said Villanueva, a 38-year-old labor organizer.
He finds refuge in his bookshelves lined with toys, a reminder of his childhood in Mexico when his father, a life insurance salesman, bought him anything he wanted. Now, it’s his parents who depend on him entirely for money, food and shelter.


“I have a 5-year-old and a teenager in the house,” he said. “The teenager is my mom, and the 5-year-old is my dad.”
Villanueva doesn’t have a plan for if things get worse — it’s hard enough maintaining as is. Maybe one day Ramon will no longer be able to get up the stairs to their second-floor apartment. But if that happens, Villanueva will probably do what he’s done for nearly a decade.
He’ll acknowledge his new reality, and adapt.
Credits: Design and development by Priya Krishnakumar